High Hematocrit and Testosterone Replacement Therapy:
What Every Man on TRT Needs to Know About Blood Thickening


Curated By Nelson Vergel | ExcelMale.com | Updated March 2026
Key Takeaways
• Hematocrit elevation is the most common dose-limiting side effect of TRT, affecting up to 66% of men on weekly injections.
• The rate of hematocrit change from your personal baseline matters as much as the absolute number -- a sharp rise doubles cardiovascular risk even if the final level looks ‘normal’.
• Delivery method is the single biggest driver of risk: intranasal testosterone causes almost no hematocrit rise, while weekly IM injections carry the highest rates.
• Therapeutic phlebotomy works quickly but can deplete iron stores -- repeated blood removal without monitoring ferritin creates a new problem.
• Sleep apnea silently compounds TRT-related blood thickening -- treating it can dramatically improve hematocrit without changing your dose.
• The clinical cutoffs most experts use: investigate at Hct >50%, intervene at >52%, and strongly consider discontinuing or doing phlebotomy above 54%.
Introduction: The Blood-Thickening Trade-Off
You started TRT and things finally clicked -- energy returned, libido improved, the gym made sense again. Then your bloodwork came back and your doctor circled one number: hematocrit. Now you’re wondering whether this therapy that’s made you feel like yourself again is quietly doing something dangerous to your blood.
This is one of the most common and important conversations in the TRT community, and it deserves a thorough answer. Elevated hematocrit -- the percentage of red blood cells in your total blood volume -- is the most frequent dose-limiting side effect of testosterone therapy. When it rises too high, blood becomes thicker and harder to pump, increasing the risk of blood clots, stroke, and heart attack. But the story is more nuanced than a single lab value. The risk depends heavily on how fast your hematocrit is rising, which formulation you use, whether you have sleep apnea, and how your individual biology responds to exogenous testosterone.
This guide pulls together current clinical research, practical protocol guidance, and insights from ExcelMale’s 20+ year community archive to give you a complete picture -- what’s happening in your body, what the numbers actually mean, when to act, and how to manage this effectively without derailing the benefits of your therapy.

Why Does Testosterone Raise Hematocrit?
The Hepcidin-Iron Connection
Testosterone doesn’t raise red blood cell counts through a single switch -- it works through several interlocking pathways. The most important starts with a protein called hepcidin, which your liver uses as the master regulator of iron. Hepcidin controls how much iron gets absorbed from food and how much circulates in your bloodstream for use by bone marrow.
Testosterone powerfully suppresses hepcidin. When hepcidin falls, iron absorption increases, more iron becomes available to the bone marrow, and red blood cell production accelerates. You can actually measure this effect by tracking soluble transferrin receptor levels -- they rise in men on TRT, confirming that the bone marrow is running in overdrive.
The EPO Set Point Reset
Here’s where things get genuinely interesting. Erythropoietin (EPO) is the hormone your kidneys produce to tell bone marrow to make more red blood cells. Normally, when hemoglobin rises, EPO falls to keep things balanced -- a classic negative feedback loop. Testosterone disrupts this feedback. Research shows that TRT essentially ‘resets’ the EPO set point to a higher level, so EPO production stays inappropriately elevated even after hemoglobin has already climbed. Your body adopts a new normal that keeps the red cell production line running.
Additional Pathways
Two other mechanisms contribute. First, testosterone converts to dihydrotestosterone (DHT) in the body, and elevated DHT levels have been independently linked to higher hematocrit, likely through direct stimulation of bone marrow precursor cells. Second, some testosterone aromatizes into estradiol, which acts on estrogen receptor-alpha in hematopoietic cells, increasing the activity of telomerase (an enzyme that helps cells replicate) and further driving red blood cell proliferation. Men with fewer CAG repeats in their androgen receptor gene appear more sensitive to these effects and more prone to significant hematocrit rises.
Why Your Delivery Method Matters More Than Your Dose
If there’s one thing the research makes crystal clear, it’s this: the testosterone molecule itself isn’t the primary problem -- the pharmacokinetic profile of how it’s delivered is. Formulations that create high peaks and low troughs push the bone marrow hardest. Those that maintain stable, physiologic levels are far gentler on blood parameters.
Think of it this way: the bone marrow responds to sustained exposure to supraphysiologic testosterone levels like a factory being ordered to run an extra shift. Weekly or biweekly intramuscular injections keep the factory in that extra shift for much of the week. Intranasal or transdermal formulations, by contrast, deliver smaller pulses the marrow largely ignores.

Sources: Pastuszak et al., Reddy et al. (2023), Middleton et al., Nackeeran et al. (2022). Rates refer to Hct >50% unless otherwise noted.
The intranasal data from Reddy et al. (2023) is particularly striking. Men using intranasal testosterone actually started with higher baseline hematocrit values (45.2%) than those on injections (41.6%) -- yet the injection group saw a sharp 4.4% increase while the intranasal group saw a slight decrease of 0.8%. Because intranasal testosterone clears quickly after each dose, it never maintains the sustained supraphysiologic exposure that drives the bone marrow to overproduce. This is a meaningful option for men who are high hematocrit responders.
Understanding Your Numbers: What the Thresholds Mean
There’s no universal agreement on exactly when elevated hematocrit requires intervention, which is part of why patients get confusing guidance. Here’s what the major organizations say and what matters most from a practical standpoint.
The Cutoff Debate
The Endocrine Society considers a hematocrit above 50% a relative contraindication to starting TRT, and recommends stopping or intervening when it exceeds 54%. Many clinical practices use 52% as their practical intervention threshold. Other societies set slightly different numbers ranging from 52% to 55%. The honest answer is that the exact upper limit hasn’t been definitively established by randomized trial data, and different clinicians apply these thresholds with different degrees of urgency.
What’s more important than any single threshold is understanding the difference between primary and secondary erythrocytosis. Primary erythrocytosis comes from a bone marrow disorder -- polycythemia vera -- and carries much higher clotting risk than secondary erythrocytosis driven by TRT or sleep apnea. When doctors apply polycythemia vera guidelines to TRT patients, they may be overstating the risk. That said, TRT-induced elevated hematocrit is not risk-free, especially in men with additional cardiovascular risk factors.
The Delta Rule: Change from Baseline Matters More Than Absolute Value
Research by Kohn and Ramasamy using data from 11,561 men revealed something important that changes how we should think about monitoring. It’s not just whether your hematocrit crosses an absolute threshold -- it’s how far it’s moved from where it started.
Men whose hematocrit went from a baseline of 44-47% up to 48-51% were twice as likely to experience a major adverse cardiac event (heart attack, stroke, or death) compared to men who stayed at their baseline levels. The risk ratio was 2.07. For men who jumped even higher -- past 52% -- the risk nearly quadrupled at 3.82. And critically, these events clustered in the first 3 to 24 months after starting TRT, which is exactly when most patients are still finding their dose.
The practical implication: if your hematocrit was 42% before starting TRT and it’s now 50%, that 8-point rise deserves attention even though 50% is technically within some labs’ reference range. Don’t just ask whether you’re ‘in range’ -- ask how far you’ve moved from your personal baseline.
Sleep Apnea: The Hidden Multiplier
If you have untreated obstructive sleep apnea (OSA) and you’re on TRT, you’ve got two independent forces pushing your hematocrit up at the same time. Sleep apnea causes repeated nighttime oxygen drops, which signals your body to produce more red blood cells to carry whatever oxygen it can find. This is the same response seen in people who live at high altitude. Combined with TRT’s direct stimulation of erythropoiesis, the cumulative effect can be substantial.
Research shows OSA severity tracks closely with hematocrit and Red Cell Distribution Width (RDW) -- a measure of variation in red blood cell size that serves as a marker of bone marrow stress and systemic inflammation. The more severe the sleep apnea, the higher these markers tend to run.
Here’s a clinical pearl that often goes unmentioned: if you’re on TRT and struggling to control hematocrit despite dose adjustments and even phlebotomy, sleep apnea testing should be on your short list. Many men are undiagnosed. Getting on CPAP therapy, or even losing weight to reduce OSA severity, can lower hematocrit meaningfully without touching your testosterone protocol.
There’s also a feedback loop worth knowing about: OSA patients on TRT tend to show lower testosterone levels on follow-up testing (around 338 ng/dL) compared to non-OSA patients on the same protocol (around 480 ng/dL). This blunted response often leads clinicians to push doses higher, which compounds the hematocrit problem further.
Managing High Hematocrit: A Practical Protocol
Step 1: Establish Your True Baseline
Before starting TRT, get a complete blood count that includes hematocrit. This baseline is your reference point for everything that follows. If you’re already on TRT and don’t have a pre-treatment baseline, look back at any bloodwork from before you started -- even a general physical -- to establish where you were.
Step 2: Monitor at the Right Intervals
Check hematocrit and hemoglobin at 3 to 6 months after starting TRT or changing your protocol. The 16-week mark is particularly meaningful because it captures the full impact of TRT on the 120-day lifespan of your red blood cells. After your levels stabilize, annual monitoring is generally sufficient unless you’re a high responder or have additional risk factors.
Always try to use the same laboratory for longitudinal comparisons. Lab-to-lab variation can be enough to cause apparent changes that aren’t real -- or mask real changes that matter.
Step 3: What to Do at Each Threshold
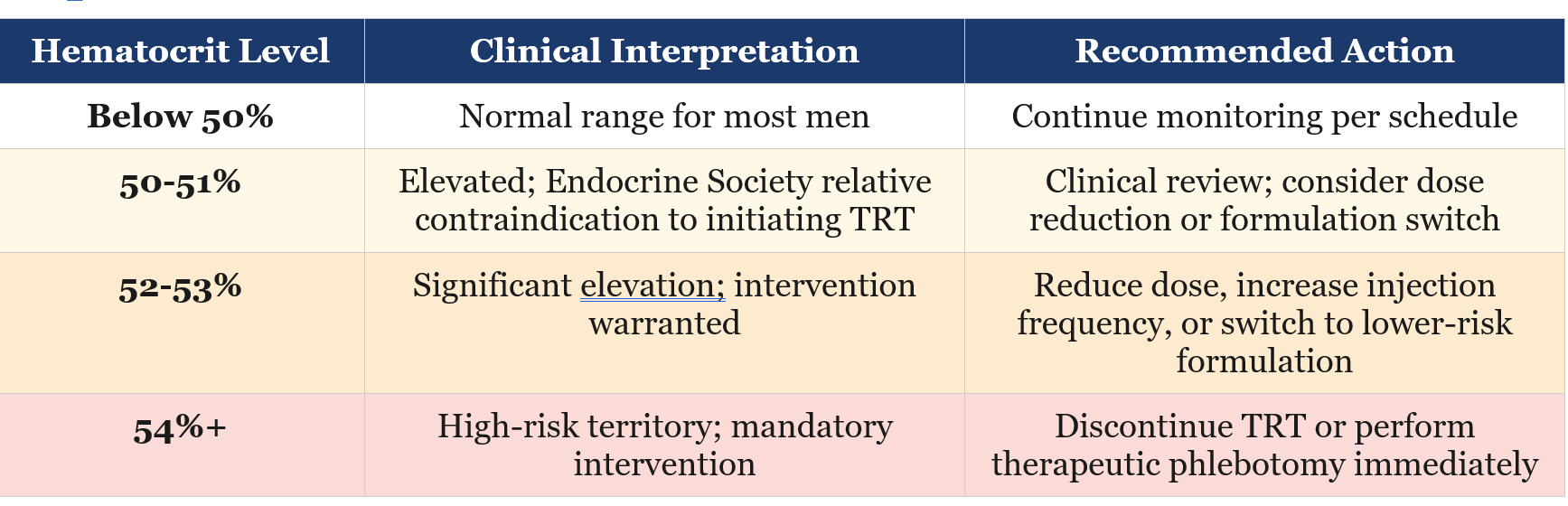
Adjusting Your Protocol Before Going Straight to Phlebotomy
Before scheduling a blood draw, consider whether changes to your TRT protocol might bring hematocrit down on their own. Splitting your weekly injection into two smaller doses (e.g., moving from 100 mg once weekly to 50 mg twice weekly) smooths out the testosterone peak and reduces sustained supraphysiologic exposure. Some men see meaningful hematocrit reduction from this simple change alone.
If you’re on weekly injections and running at 52-53%, switching to transdermal gel or oral testosterone may be worth discussing with your doctor -- especially if the switch fits your lifestyle and you can tolerate the application routine. Intranasal testosterone is worth considering for men who are clear high responders.
Ensure you’re well-hydrated before bloodwork. Dehydration can artificially inflate hematocrit readings by concentrating the blood. Drink well the day before your lab draw and don’t exercise vigorously the morning of the test, as exercise temporarily shifts fluid out of the vascular space.
Therapeutic Phlebotomy: Benefits, Limits, and the Iron Problem
When hematocrit reaches 54% or higher -- or when protocol adjustments haven’t been enough -- therapeutic phlebotomy becomes necessary. One unit of blood (approximately 500 mL) removes roughly 200-250 mg of iron and typically drops hematocrit by about 3 percentage points. The procedure is the same as blood donation and can often be done at a blood bank with a physician’s order.
Here’s where many men run into an unexpected complication: repeated phlebotomies deplete iron stores. Since testosterone has already suppressed hepcidin and increased iron turnover, the combination of high iron demand from elevated red blood cell production and repeated iron removal from phlebotomy can drive ferritin into deficiency territory. You can end up with low ferritin and fatigue even while your hematocrit remains elevated -- a frustrating paradox the ExcelMale community has discussed extensively.
A 2024 Dutch paper by Bond, Verdegaal, and Smit raised another concern worth knowing: phlebotomy lowers tissue oxygen levels, which may activate HIF (hypoxia-inducible factor) pathways that could paradoxically increase EPO and further stimulate red blood cell production. This doesn’t mean phlebotomy is wrong -- it often is necessary -- but it means that treating the symptom without addressing the root cause (usually dose or formulation) puts you on a treadmill. Monitor ferritin alongside your CBC, and discuss iron supplementation with your physician if ferritin falls below 30 ng/mL.
For blood donation specifically, be aware that repeat donations may not be sufficient to maintain hematocrit below 54% in high responders. A Canadian study found that 44% of TRT patients who donated blood regularly still had persistently elevated hemoglobin at subsequent visits. Donation is a useful tool but not a complete management strategy by itself.
Who Is at Highest Risk?
Not every man on TRT develops significant hematocrit elevation. Certain factors consistently predict higher risk:
• Injection formulations, especially weekly or biweekly dosing of testosterone cypionate or enanthate.
• Older age at the time of initiating TRT -- likely due to reduced plasma volume and lower baseline EPO regulation.
• Obesity (BMI above 30) -- associated with baseline erythropoietic dysregulation.
• Smoking -- smokers’ polycythemia is a well-recognized phenomenon independent of TRT.
• Untreated or severe obstructive sleep apnea.
• Chronic lung conditions such as COPD, asthma, and chronic bronchitis -- all cause hypoxia that drives erythropoiesis.
• Higher baseline hematocrit before starting TRT -- if you’re already at the upper end of normal, there’s less room before you cross a threshold.
• Genetic predisposition -- men with fewer than 20 CAG repeats in the androgen receptor gene appear more sensitive to testosterone’s erythropoietic effects.
If several of these factors apply to you, your physician should discuss formulation choice explicitly at the start of TRT rather than waiting to see what happens. Starting a high-risk patient on weekly injections and then managing the fallout reactively isn’t optimal care.
What ExcelMale Members Have Learned
The ExcelMale forum has accumulated over two decades of real-world experience with hematocrit management. A few consistent themes emerge from the community that complement what clinical research shows:
Many members report that switching from once-weekly to twice-weekly injections (splitting the same total dose) noticeably reduced hematocrit over several months. This matches the clinical logic: smoothing out the peak reduces sustained supraphysiologic exposure. The change doesn’t require lowering your total weekly dose.
The ferritin depletion problem from frequent phlebotomy is widely discussed and often underappreciated by physicians unfamiliar with TRT management. Members frequently note that fatigue after repeated donations isn’t just the expected post-donation tiredness -- it can reflect genuine iron deficiency that needs to be addressed before the next phlebotomy cycle. Checking ferritin every 2-3 months when undergoing frequent phlebotomy is standard community practice.
There’s ongoing debate in the community about how aggressively to treat hematocrit in the 50-53% range in men who feel fine and have no other cardiovascular risk factors. Some members report being managed conservatively at levels their doctors consider borderline, with close monitoring rather than intervention, and doing well. The ExcelMale forum thread on this topic reflects the real clinical uncertainty that exists even among experienced practitioners -- the evidence at these borderline levels is genuinely ambiguous.
The emerging interest in rusfertide -- a synthetic hepcidin being studied for polycythemia vera -- has caught the community’s attention as a potential future option for men whose hematocrit keeps rebounding after phlebotomy. It’s not approved for TRT-related erythrocytosis and would likely require off-label use, but the mechanism is directly relevant: if TRT suppresses hepcidin and that drives the problem, restoring hepcidin-like activity could address the root cause.
Getting Your Doctor on Board
One challenge many men face is physicians who either dismiss hematocrit concerns or overreact to modest elevations. A few strategies that help:
• Bring your baseline hematocrit to every appointment and ask your doctor to evaluate the change, not just the current value.
• If your doctor wants to order phlebotomy, ask whether a formulation switch or dose adjustment should be tried first -- this addresses the cause rather than just the symptom.
• If your hematocrit is high and you have any symptoms of sleep apnea (snoring, morning headaches, daytime fatigue, witnessed breathing pauses), push for a sleep study before assuming TRT dose is the only issue.
• Ask for ferritin to be included in your monitoring panel, especially if you’re undergoing regular phlebotomy. Iron deficiency anemia in the setting of elevated hematocrit is a real paradox that requires its own management.
• If you’re getting therapeutic phlebotomy, let your doctor know the specific dates and volumes so it can be factored into the next lab interpretation.
The Bottom Line
Elevated hematocrit is a manageable aspect of TRT -- not a reason to give up on therapy that’s improving your quality of life, but also not something to wave away because you feel fine. The absence of symptoms doesn’t mean the absence of risk.
The most important things you can do: know your baseline, watch the rate of change, choose a formulation that fits your risk profile, rule out sleep apnea if your numbers keep climbing, and don’t treat phlebotomy as a substitute for addressing the underlying cause. Men who take an active, informed role in their own monitoring tend to do far better than those who just wait for their doctor to flag a problem.
ExcelMale has always been about giving men the information they need to have a real conversation with their healthcare providers -- not to self-treat, but to participate as partners in their own care. Your hematocrit is one of the most important numbers to understand on TRT. This guide gives you the foundation to do exactly that.
Related ExcelMale Forum Discussions
Explore these community discussions for additional insights:
How to Lower High Hematocrit Caused by Testosterone Replacement Therapy (TRT)
Nelson Vergel’s comprehensive overview covering mechanisms, monitoring protocols, and practical management strategies for TRT-induced hematocrit elevation.
Controlling the Polycythemia Effect Associated with TRT
Discussion of clinical strategies for minimizing secondary polycythemia, including how dose stability affects hematocrit trajectories over time.
Is It True That an Elevated Hematocrit on TRT Does Not Require Blood Donation?
A nuanced community debate about the clinical significance of borderline hematocrit elevations, including perspectives from experienced TRT practitioners and patient advocates.
Where to Get Therapeutic Phlebotomies to Lower High Hematocrit in the U.S.
Practical guide from members on locating therapeutic phlebotomy services, understanding FDA donor eligibility rules for TRT patients, and working with blood banks.
Member experiences and clinical perspectives on the real cardiovascular risks of sustained hematocrit elevation, including the debate between absolute thresholds versus rate of change.
Rusfertide Decreases Need for Therapeutic Phlebotomy in Polycythemia Vera
Coverage of emerging research on rusfertide (a synthetic hepcidin) and its potential relevance for men on TRT who struggle with recurrent hematocrit elevation despite phlebotomy.
Effective Strategies: How to Lower Hematocrit on TRT
Member-tested approaches including injection frequency adjustments, hydration strategies, formulation changes, and monitoring tips for managing hematocrit long-term.
How to Lower Red Blood Cell Count and Hematocrit While on Testosterone
Detailed review of hematocrit management strategies for TRT patients, with attention to the interplay between red blood cell count, hemoglobin, and hematocrit measurements.
Key References
1. Bond P, Verdegaal T, Smit DL. Testosterone therapy-induced erythrocytosis: can phlebotomy be justified? Endocrine Connections. 2024 Sep;13(10):e240283.
2. Liu J, et al. Diagnosis, management, and outcomes of drug-induced erythrocytosis: a systematic review. Blood Advances. 2025;9(9):2108-2118.
3. Kohn TP, Agrawal P, Ory J, Hare J, Ramasamy R. Rises in Hematocrit Are Associated With an Increased Risk of Major Adverse Cardiovascular Events in Men Starting Testosterone Therapy. Journal of Urology. 2024;211(2):285-293.
4. Nackeeran S, et al. The Effect of Route of Testosterone on Changes in Hematocrit: A Systematic Review and Bayesian Network Meta-Analysis of Randomized Trials. Journal of Urology. 2022;207:44-51.
5. Nguyen CP, Hirsch MS, Moeny D, et al. Erythrocytosis Following Testosterone Therapy. PMC Review Article. Sexual Medicine Reviews.
6. Neidhart A, von Wyl V, Kaslin B, Henzen C, Fischli S. Prevalence and predictive factors of testosterone-induced erythrocytosis: a retrospective single center study. Frontiers in Endocrinology. 2025 Jan 15;15:1496906.
7. Okano S, et al. Effect of testosterone formulations on hematocrit in transgender individuals: A systematic review. Andrology. 2025.
8. Graydon RJ, et al. Blood donation and testosterone replacement therapy. Transfusion. 2017;57(2):252-256.
9. Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism. 2018;103(5):1715-1744.
10. Fink J, Bentzen K, Horie S. Management of hematocrit levels for testosterone replacement patients, a narrative review. Sexual Medicine Reviews. 2025;13(2):229-236. doi:10.1093/sxmrev/qeaf013.
Medical Disclaimer
This article is for educational and informational purposes only. It does not constitute medical advice and should not replace a consultation with a qualified healthcare provider. Hematocrit management on TRT requires individualized clinical evaluation. Always discuss any changes to your testosterone protocol with your prescribing physician before making adjustments.
About ExcelMale.com
ExcelMale.com is a men’s health forum with over 24,000 members and a 20+ year archive of evidence-based discussions on testosterone replacement therapy, hormone optimization, sexual health, and men’s wellness. Founded and curated by Nelson Vergel -- author of Testosterone: A Man’s Guide and Beyond Testosterone, and a 30+ year patient advocate in men’s hormone health -- ExcelMale bridges peer-reviewed clinical research with real-world patient experience. Visit us at ExcelMale.com.